Dr Alison Pearce has won a Best New Investigator Presentation Award at the Annual European Congress of the International Society for Pharmacoeconomics and Outcomes Research (ISPOR). The award recognises the scientific merit of a podium presentation at the conference, which was held in Milan, Italy.
The award was given for Alison’s work which found that lost productivity due to cancer in Brazil, Russia, India, China and South Africa costs around $47 billion US dollars annually.
When people die from cancer, their contribution to society through paid work, called productivity, is lost. Over 70% of cancer deaths in the world occur in developing countries, and Brazil, Russia, India, China and South Africa (the BRICS countries) are the most rapidly developing economies in the world. The results highlight the importance of tobacco control, vaccination for hepatitis, and improved access to early detection and treatment in developing countries.
The National Cancer Registry is leading this research with a group of collaborators from around the world, including the International Agency for Research on Cancer (IARC) in France and researchers in Ireland, the UK, Brazil, Russia, India, China and South Africa. ISPOR is a non-profit, international, educational and scientific organisation that promotes health economics and outcomes research excellence to improve decision making for health globally.
This news item was originally published on the National Cancer Registry Ireland website: http://www.ncri.ie/news/article/dr-alison-pearce-health-economist-registry-wins-prestigious-conference-award
Cancer deaths in Brazil, Russia, India, China and South Africa (the largest emerging economies in the world) result in over $51 billion (USD) in lost productivity each year. These results are being presented at an international conference in India today.
Researchers at the National Cancer Registry Ireland (NCRI) have estimated that lost productivity due to cancer deaths costs China over $28 billion each year, followed by India ($6.7 billion), Russia ($5 billion), Brazil ($4.6 billion) and finally South Africa ($2.8 billion) each year.
When people die due to cancer, their contribution to society through paid work, called productivity, is lost. Over 70% of cancer deaths in the world occur in developing countries, and Brazil, Russia, India, China and South Africa (together known as the BRICS countries) are the most rapidly emerging economies in the world. Leading an international collaboration of researchers, the NCRI have been investigating productivity loss in the BRICS countries.
The analysis shows cancers related to tobacco contribute between 27% (South Africa) and 38% (India) of productivity losses across the BRICS countries. Over half of men in Russia and India smoke, and it is clear that anti-tobacco legislation is an important part of cancer control in the BRICS countries.
The analysis also shows the potential importance of vaccinations for hepatitis and HPV in BRICS countries. Cancers such as liver cancer, cervical cancer and head and neck cancers are all preventable with these vaccinations, but continue to have a high impact on lost productivity in BRICS countries.
These results are being presented today at the annual conference of theInternational Association of Cancer Registries (IACR). The conference is being held in Mumbai, India, and aims to provide people working in cancer registries with a forum for learning and exchanging ideas. The work has been done with a group of international collaborators, including from the International Agency for Research on Cancer (IARC) in France, and researchers in Ireland, the UK, Brazil, Russia, India and China.
This news item was originally published on the National Cancer Registry Ireland website: http://www.ncri.ie/news/article/registry-research-costs-cancer-be-presented-international-conference-india
After treatment for prostate cancer, men have ongoing follow-up to monitor for the cancer returning, and to manage any treatment side effects. Traditionally, this follow-up is done by specialist clinicians in the hospital setting, but the growing number of prostate cancer survivors means this is not sustainable.
Evidence suggests that follow-up by a GP, instead of a specialist clinician, doesn’t change how long people survive, how many cancers are identified, or quality of life for cancer survivors. However, the costs of GP-led prostate cancer follow-up have not been investigated in Ireland.
Health economists at the National Cancer Registry Ireland (NCRI) have developed an economic model comparing the health system costs of three strategies for prostate cancer follow-up in Ireland:
The European Association of Urology (EAU) guidelines, which recommend traditional follow-up by a hospital-based specialist.
The National Institute of Health Care Excellence (NICE) guidelines, which recommend well patients are followed up by GPs after two years.
Current practice in Ireland, based on an NCRI survey.
The results, published in the journal Supportive Care in Cancer, showed that the GP-based follow-up in the NICE guidelines is the most cost efficient strategy for prostate cancer follow-up. Current practice is the least cost efficient strategy because it includes duplication of services within the hospital and primary care. If all the men diagnosed with prostate cancer in Ireland in 2013 were offered follow-up according to the NICE guidelines for the next 10 years, the Irish health care system could save more than €760,000.
Identifying an efficient and sustainable strategy for prostate cancer follow-up care could help to reduce the growing strain on the health care budget. While economic models are simplifications of reality, these results suggest that moving prostate cancer follow-up to primary care should be considered in Ireland to improve efficiency and sustainability.
This work is part of a larger program of research investigating the Challenges of Cancer Survivorship in Ireland funded by the Health Research Board (HRB) and conducted at the National Cancer Registry Ireland in collaboration with national and international researchers.
This news item was originally published on the National Cancer Registry Ireland website: http://www.ncri.ie/news/article/prostate-cancer-follow-gps-more-efficient-hospital-based-care
Dr Alison Pearce has won a Young Investigator of the Year Award at the Annual Meeting on Supportive Care in Cancer, hosted by the Multinational Association of Supportive Care in Cancer (MASCC) and the International Society of Oral Oncology (ISOO). The Young Investigator of the Year Awards recognise outstanding young investigators’ research accomplishments.
The award was given for Alison’s work with Ms Fay Ryan, a health economist who completed her Masters project with the National Cancer Registry in 2014. Their project looked at the costs of prostate cancer follow-up care in Ireland as part of the Challenges in Cancer Survivorship project.
Prostate cancer follow-up care is traditionally provided by clinicians in hospital settings. However, growing numbers of prostate cancer survivors mean this may not be economically sustainable and a number of alternative approaches have been suggested. Alison and Fay compared the costs of three alternative strategies for prostate cancer follow-up care in Ireland.
The results indicate that following the UK-based National Institute of Health and Care Excellence (NICE) Guidelines was the most cost efficient follow-up strategy, because NICE recommend follow-up care of well patients be conducted by General Practitioners (GPs) after 2 years, rather than continuing to see hospital-based clinicians. Alison and Fay estimated that the Irish health care system could have saved €760,000 over a 10-year period if the NICE guidelines were adopted in Ireland.
This was the first study investigating the costs of prostate cancer follow-up in the Irish setting, and Alison and Fay’s work was ranked in the top 10 abstracts by junior investigators submitted to the conference, which was held last week in Copenhagen.
This news item was originally published on the National Cancer Registry Ireland website: http://www.ncri.ie/news/article/research-costs-cancer-follow-wins-conference-award
When people take time off work because of cancer, society loses their contribution to the economy. Our new study looks at different ways of valuing this contribution.
Most people with cancer take some time off work for treatment, recuperation and rehabilitation. As well as impacting on a person’s sense of identity and quality of life, this time away from work has implications for society, because each individual in the workforce contributes to the economy. This contribution to the economy is known as productivity. Estimating the productivity lost due to a disease can help with health care service planning and policy making.
This study estimated the productivity lost due to time off work and premature mortality from head and neck cancer in Ireland using two different methods. Both methods found that productivity losses following head and neck cancer are substantial, and are higher than seen in other cancers. For each working person diagnosed with head and neck cancer, the first method found that society loses on average €253,800, while the second approach found that on average society loses €6,800.
The two methods had very different results because they have different assumptions about what is included in lost productivity. For example, if someone retires early because of cancer, the first method includes a value for each year until they should have retired. In contrast, the second method only includes the time it takes until their position has been filled.
These contrasting results highlight that using different methods to estimate the impact of a disease on the economy can have very different results. At the moment, there is no consensus on the best method to use. Our research suggests that using both approaches, as we have done, is a good way of estimating the range of the potential productivity losses.
This news item was originally published on the National Cancer Registry Ireland website: http://www.ncri.ie/news/article/cost-society-time-work-after-head-and-neck-cancer
A new paper published in the Journal of Cancer Survivorship by researchers at the National Cancer Registry investigates the patterns of return to work in people with head and neck cancer.
The study looked at people diagnosed with head and neck cancer who had been working at the time of diagnosis. It found that while most people (77%) took some time off work for treatment and recovery, over half of people (58%) eventually did return to work after their diagnosis. The average time taken off work was 9 months, but a small group of people were absent for more than a year before they returned to work. Factors such as the type of cancer, type of treatment and type of work someone had all influenced chances of returning to work after head and neck cancer.
This is the first study to provide estimates of the proportion of people who take time off work following a diagnosis of head and neck cancer and the findings are important for patients, clinicians and employers.
Working contributes to an individual’s sense of self and quality of life, as well as protecting against financial distress, therefore it is important that head and neck cancer survivors are aware that return to work is possible, but may take an extended period of time.
Clinicians need to be aware that patients’ future workforce participation should be considered from the time of diagnosis and may continue to be an issue during and beyond the period of rehabilitation. Policy makers and employers need to be aware that flexibility is required in the workplace to accommodate longer term effects following head and neck cancer, as may be occupational rehabilitation.
This news item was originally published on the National Cancer Registry Ireland website: http://www.ncri.ie/news/article/returning-work-after-head-and-neck-cancer
Cancer rates are set to double in Ireland by 2040 – here’s why
By Alison Pearce, National Cancer Registry Ireland and Harry Comber, National Cancer Registry Ireland
The latest projections from the National Cancer Registry show that the number of new cancer cases being diagnosed each year in Ireland is expected to double by 2040. To understand such a dramatic rise we need to look a bit more deeply at how the figures are calculated. Three elements determine the projection of trends in cancer incidence: population change, cancer trends, and changes in exposure to risk factors.
Projected numbers of all invasive cancers in Ireland, excluding non-melanoma skin. NCRI
Population change
An ageing population is the main factor driving an increase in cancer numbers. This is because the rate of ageing is much bigger than any changes in the rate of cancer.
The NCR projections use models of population change provided by the Central Statistics Office. These models make a number of assumptions about mortality, migration and fertility. Only the first of these is likely to have any major impact on future cancer numbers, as the others affect the younger population, where cancer cases are low. With the ageing of the population, and improved life expectancy, the median age of cancer patients at diagnosis will increase.
The projections indicate that almost 50% of people with invasive cancers will be aged over 70. As a result there will not only be more cancer patients, but they will be older on average.
Cancer trends
The projections are also based on the assumption that current trends in cancer incidence will continue. For each cancer, we examined the incidence rates from 1994 to 2010 to find the current trend.
Non-melanoma skin cancer rates, for example, have been increasing since 2001. The projections show that this increase will continue in the future, and skin cancers will in fact be the most rapidly increasing cancers in the future. The primary risk factor for non-melanoma cancer of the skin is UV exposure, and evidence suggests that this steady increase is mainly due to recreational UV exposure, such as sunbeds.
But it doesn’t always follow that what is happening now will predict what will happen in the future. The rapid increase in prostate cancer cases in the 1990s and early 2000s, for example, was due to the widespread use of Prostate Specific Antigen (PSA) testing. This is a blood test which measures the level of the PSA protein in the bloodstream, and was introduced as a way to help with the diagnosis of prostate cancer. But this trend began to level off around 2004, when PSA testing was found to be less useful that previously thought, because many people with raised PSA levels do not have prostate cancer and some prostate cancers identified through testing are very slow growing and may not require treatment. Because of the large variations in trend for prostate cancer in the past two decades, the projections aren’t regarded as very reliable.
Another example of something that can affect cancer rates and therefore projected trends is screening. The introduction of screening for breast and cervical cancers led to a considerable increase in the number of cases that were diagnosed. Screening for colorectal cancer recently begun in Ireland and novel methods of screening for other cancers will probably appear in the next decade. While some screening may eventually bring about a reduction in health service costs, screening will initially increase case numbers and costs above what might be expected from natural increase.
Lifestyle factors
Four risk factors have been shown to determine the majority of the attributable risk of cancer (excluding non-melanoma skin cancer) in the UK: tobacco, diet (including food energy balance, obesity and physical activity), alcohol and reproductive factors. Three of these can be considered lifestyle-related. There are no equivalent calculations for Ireland, but given the similarity in lifestyle between the populations of Ireland and the UK, it is reasonable to assume that the distribution and prevalence of attributable risks due to these major factors are similar.
The link between exposure to these risk factors and cancer incidence can perhaps be most clearly seen with tobacco smoking. Smoking has been implicated as a causal factor in many cancers, and is the cause of the overwhelming majority of lung cancer cases. Smoking prevalence in Ireland is high, although decreasing slowly, and more rapidly in males than females. Overall there has been a fall of about 9% in smoking prevalence for males and of about 8% for females since 1986.
Cigarette smoking preference by gender – 12-month moving average to June 2012. Office of Tobacco Control, Ireland
The estimated increase in tobacco-related cancers in Ireland and between 2010 and 2040 is 110-115% in females and 83-91% in males. However, given the gradual decrease in female smoking rates in the 1990s, there is likely to be an eventual levelling-off in the number of female lung cancer cases. Men have much higher smoking rates overall, so although it is falling for both genders, it will still take longer for male rates to catch up.
What all this shows is that projections of cancer cases based on existing trends are limited in their ability to predict the future cancer burden. However, the overall conclusions from these projections are clear. Although we cannot modify the effects of demographic change, the majority of cancer risk is due to a small number of well understood and potentially modifiable behaviours: UV exposure, smoking, alcohol consumption, diet and exercise.
Alison Pearce receives funding from the Health Research Board.
Harry Comber does not work for, consult to, own shares in or receive funding from any company or organisation that would benefit from this article, and has no relevant affiliations.
A review of the premature mortality costs associated with cancer has found that these costs are substantial, and appear to be rising.
Premature mortality costs are one component of the societal impact that cancer has on the economic health of a country, on top of the obvious population health burden. These costs to society are related to lost productivity – the time lost from usual activities such as work, household activities, caregiving and voluntary work – that occur when an individual dies prematurely from cancer.
Researchers from the National College of Ireland and the National Cancer Registry Ireland conducted a review of recent studies of premature mortality costs. In all settings considered, the costs of premature cancer-related mortality were substantial, and appeared to be increasing. Of note, the ‘true’ societal costs were often underestimated, as unpaid work such as household activities, caring and volunteer work were not included.
The review identified that improvements in the quality and quantity of cancer-related premature mortality cost estimates are required, as increased awareness of the societal impacts of cancer can inform health policy makers.
This news item was originally published on the National Cancer Registry Ireland website: http://www.ncri.ie/news/article/review-finds-costs-cancer-related-premature-mortality-are-rising
When doing economic evaluation you often need to forecast into the future. And when projecting about earnings, you need to account for changes in the economy (for example, inflation). I am currently working on a study examining productivity losses associated with cancer in Ireland, and need to account for wage growth in the future. But how do you do this when the economy is as uncertain as the current situation in Ireland?
Wage growth: This Wall Street Journal blogpost describes wage growth as one of the key indicators of economic health (as well as some of the current problems with wage growth in the US). In Ireland there are similar economic woes, but future predictions of the real wage growth rate are harder to come by. Instead, people have used the Gross National Product (GNP) percentage change per year as a proxy for wage growth. GNP is the total value of all products and services produced by residents of a country over a particular period of time. Previous work similar to mine (Hanley 2012 & Hanley 2013) has used older versions of these predictions, which estimated an average growth rate of 2.6%.
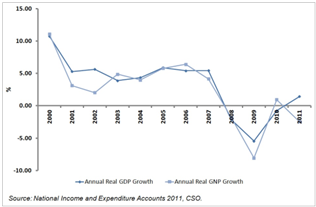
GNP in Ireland: At the height of the Celtic Tiger period (mid 1990’s to mid 2000’s) GNP in Ireland was over 5%, however in the period 2007 to 2012 the growth rate of GNP in Ireland has been -2.2%. The Economic and Social Research Institute (ESRI) propose that this was due to the global financial crises causing the Irish housing market to crash. This in turn led to collapse of the construction and banking industries, resulting in Ireland entering a period of recession. This period has been characterised by high levels of state debt and unemployment.
GNP growth projections: According to the latest report from ESRI, the GNP growth rate in coming years will be dependent on a number of factors, particularly the recovery of the EU economy, domestic policy decisions and the impact of changes in both the EU and Irish economies on domestic government finances. The report explains that the current government policy-making position is a risk averse one of ‘no regrets’. Although not necessarily resulting in the ‘optimal’ policy option being selected, this approach should result in policy options which lead to generally positive outcomes across a range of possible scenarios being selected / implemented. This is necessary given the current tenuous position of the Irish economy to withstand any additional shocks, as well as the high level of uncertainty in the economic environment both locally and more broadly in the EU and worldwide.
The ESRI report includes estimates of GNP growth rates in the medium term (2015 to 2020) under three recovery scenarios, ranging from stagnation to recovery. See table below for summary of GNP growth under the three scenarios.
% GNP Change per year
Scenario
2012
2013
2014
2015
2016
2017
2018
2019
2020
Recover
3.3
1.2
0.5
4.3
3.6
4
3.4
3.2
3.6
Delayed adjustment
3.3
1.3
-0.9
3
1.1
2.8
3.1
–
–
Stagnation
3.3
1.2
0
1.9
0.6
2.1
0.4
0.9
1.7
This report provides an ideal source for the proxy wage growth estimates, as it takes into account many aspects of economic recovery you might not have considered. For the calculation of productivity losses associated with cancer in Ireland, you could use the wage growth rate based on the forecast GNP growth rate from the recent ESRI report. You can use the Delayed Adjustment scenario as the base case, with the Recovery and Stagnation scenarios providing upper and lower bounds for sensitivity analysis.
Extra considerations: If using this, you need to be aware of a number of considerations:
You could calculate the growth adjustment per year for each year of lost productivity, or use the average of the annual % change for the years 2015 – 2030. For my work, the changes between years are less important, and I will use the average.
The wage growth rate may not be consistent with reports of other improvements in the economy, making GNP growth a poor proxy. This was well described in the Wall Street Journal article mentioned earlier, which discusses how the current pattern of economic recovery in the US is masking consistently low real wage growth rates. In this case, you must weigh up using current real wage growth (which may not hold for the future) against using a potentially poor proxy but which has been projected to take account of the changing economic environment. For my research, I believe that the uncertainty around economic recovery scenarios is more important than the potential difference between actual wage growth and the proxy value, so I am going to use the projected GNP growth.
As with any projection or forecast or prediction, it is almost certainly wrong! So you need to carefully consider the uncertainty around the estimates and how they might influence your results.
Overall, this is a difficult economic time to be trying to make forecasts, however the very useful report from ESRI gives a good platform on which to form a base case and sensitivity analysis. And remember, the most important component of choosing a growth rate (or any assumption in your model) is to have a justification for your choice of methods and sources.
I am attending the International Society for Pharmacoeconomics and Outcomes Research (ISPOR) conference in Dublin on the 2nd to the 6th of November. As part of this I am presenting two posters related to my PhD.
As well as these being available at the conference and on the ISPOR website, I am making these available here via QR code.
If you are interested in the posters please feel free to get in touch, or if you are the conference come and say hi during the poster discussion hour on Monday evening.