This is a guest blogpost by Marjon Faaij, who I was delighted to supervise for her Master of Pharmacy research project. We made a great team – Marjon had a personal interest in the impact of cancer on daily life, and I had access to some data about cancer survivorship through the PROFILES registry. Even better, because Marjon was from Utrech University, she could translate the Dutch PROFILES data much more easily than I could! Marjon presented the results of her research at the NCRI conference in the UK, and we are now writing them up as a publication. In the meantime, Marjon put together this summary, and was kind enough to let me share it here.
In 2005, I lost my mother due to cancer. Before she died, she was sick for almost three years. During this period, cancer had a big impact on her daily life. Shortly after the diagnosis of cancer she could still do everything she liked; working in the hospital as a nurse, taking care of her family, cleaning our house, giving music lessons and swim lessons and socialising with friends and family. But as the time after the diagnosis increased, she became sicker, she had more pain and was more tired. She did not have the energy to do all the things she liked. She decided to work less hours until she stopped working completely. She used this time to spend more time with us and to rest more.
A lot of different factors influenced her decisions about doing work, unpaid work and leisure. One of the most important factors for her was the support from family and friends, but I can imagine that it will be different for each cancer patient.
Therefore, I decided to do a research project about the different factors of influence on cancer survivors doing daily activities, for my Master of Pharmacy. For this research I used surveys of Dutch cancer survivors, including people with Hodgkin lymphoma, non-Hodgkin’s lymphoma, multiple myeloma, thyroid or prostate cancer.
Factors of influence
From my results it is clear that cancer survivors are less likely to do paid work, and those who do work are likely to work fewer hours. Cancer survivors are also more limited in their unpaid work and leisure. However, how much cancer influences each activity is dependent on cancer type. Each cancer type has different symptoms, and has different treatments, which leads to different influence on doing daily activities.
Consistent to my mother, most cancer survivors try to keep working and fully participate in leisure and unpaid work activities. However, if they become sicker it is harder to fully participate in these activities. When they are limited in one area, they appear to be limited in all activities.
There are a lot of factors that have influence on doing daily activities. For example:
– People were less likely to have a paid job if they were: female, had surgery, older, widowed or had multiple comorbidities.
– People were more likely to be limited in their unpaid work if they had: non-Hodgkin lymphoma or multiple myeloma, multiple comorbidities, were female, or were never married.
– People were more limited in their leisure activities if they had: medium education or multiple comorbidities.
It was interesting that people who received more follow-up services were no more or less likely to report difficulty with paid work, unpaid work or leisure. But people who felt satisfied with the follow-up care they received had an increased chance of participating in daily activities.
What does this mean?
These results show that there are many factors of influence on daily activities. The factors are unique for each cancer survivor, and so are the impacts. It is important for patients to know that changes can take place across all of their daily activities during cancer, so they can prepare for and react to these changes.
Doctors need to know that cancer and its treatment can influence patients’ daily activities, and that these changes can be important for quality of life. Discussing these changes with patients and providing support and referral to services that can assist patients (and their families) during this difficult time. These referrals are not possible if there is nowhere to refer patients to, and so health care systems need to ensure that services like work rehabilitation, occupational therapy and palliative care are available and appropriately funded.
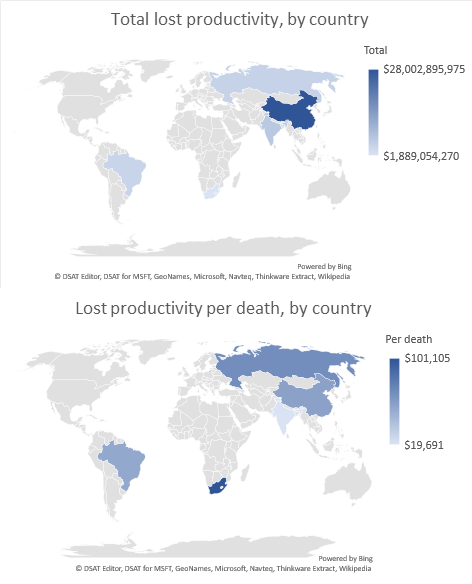
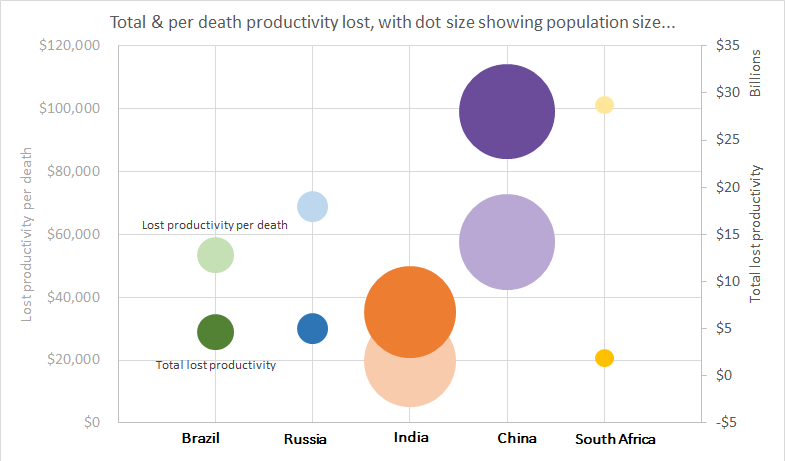
Finally, the results are important for health economics. Economic evaluation using a societal perspective account for changes in paid work due to illness (known as lost productivity) but the contribution of unpaid work usually goes unaccounted for. From these results it is clear that cancer has a big impact on both paid and unpaid work, and thus both should be considered in economic evaluations taking a societal perspective.
This research, cancer is about more than health – work and leisure after cancer, is based on data of the PROFILES Registry. This research project is carried out by Marjon Faaij. She is a Dutch Master of Pharmacy student from Utrecht University. This research project has been done at the Centre for Health Economics Research and Evaluation at the University of Technology Sydney, under the supervision of Alison Pearce and in collaboration with Dounya Schoormans of the PROFILES Registry.




 I was thrilled to be awarded the Overall winner of the 2018
I was thrilled to be awarded the Overall winner of the 2018 

{kind=link}