I’m very excited to share our new paper, showing Australian women are divided on the use of artificial intelligence (AI) in breast cancer screening. While AI has the potential to enhance the accuracy of mammogram reviews and reduce healthcare costs, many women remain sceptical.
Our study, which used a discrete choice experiment to survey over 800 Australian women, sought to understand their feelings about this technology and whether it would affect their participation in breast cancer screening.
There were mixed reactions about using AI in breast cancer screening. 40% of respondents were open to using AI if it proves more accurate than human radiologists. However, 42% were strongly opposed, and 18% had reservations that need addressing.
If it is going to be implemented, women want the AI to be accurate, Australian-owned, representative of Australian women, and faster than human radiologists. We saw that up to 22% of respondents might reduce their participation in breast cancer screening if AI is implemented in a way that makes them uncomfortable.
This supports what we see in other countries. In particular, people expect AI systems to have strong evidence they perform better than current systems before implementation. This evidence is currently not available, suggesting that implementing AI now could undermine trust in breast cancer screening programs.
I attended the Australian Occupational Therapy Conference last week, for the first time in nearly 15 years! I went to support some OT’s I’ve been working with on an economic evaluation, but it was lovely to catch up with friends and colleagues from my OT life before health economics. I also realised there wasn’t much health economics at the conference, and I got a few requests for some introductory resources about health economics. So, I’ve put together a brief summary of what health economics is and how it could apply to occupational therapy.
In general, health economics is about how we allocate our scarce health resources to maximise our health outcomes. There can be a misconception that economics is about cutting costs. But health economics is really about value, and therefore the benefits that can be achieved are just as important to a health economist as the costs of achieving them.
Everyone uses economic thinking in their daily lives – I recently bought a new laptop and had to work out which aspects of performance I would prioritise (memory, touch screen, processing power) to get a laptop within my budget (my constrained resources). For some great examples of how economic theory plays out in real life then I highly recommend the Freakonomics podcast! There are some episodes specific to health, such as Are you ready for a glorious sunset and How many Doctors does it take to start a healthcare revolution and How do we know what really works in healthcare, but all the episodes will teach you to think like an economist.
For a more formal reading, there is a paper by Kernick (2003) Introduction to health economics for the medical practitioner that gives a nice introduction to health economics, and the types of questions that health economists try to answer. If you want a bit more about some important economic concepts such as opportunity costs and marginal costs, then Goodacre & McCabe’s (2002) An introduction to economic evaluation and this Sanofi factsheet (2009) on What is health economics are other good resources.
You will notice that these papers talk in general about health economics, and then go straight into a discussion of economic evaluation. Economic evaluation is probably the most common method associated with health economics and is used world-wide (including by the PBS and MBS in Australia) to evaluate the cost-effectiveness of new interventions. An economic evaluation compares two (or more) interventions in terms of both the costs and the benefits. Economic evaluations are typically trial-based (meaning they are embedded in a clinical trial) or modelled (meaning they are based on research from the literature), or a combination of both.
The previously mentioned readings are good introductions to economic evaluations, and also explain the difference between a cost-benefit, cost-effectiveness and cost-utility analysis. These terms are often used interchangeably, but in health economics they have specific meanings based on the outcome measure you are using.
But… health economics is much more than economic evaluations. Health economists are interested in questions like: what influences health (other than healthcare), what is ‘health’ and how do we value it, how can we arrange the health workforce most efficiently, how does the way we pay doctors change their performance, how can we make health more equitable, and many more (see Alan William’s famous ‘Plumbing Diagram‘). Some of the questions I am using economic approaches to answer include:
How do we quantitatively measure patient preferences for health and health care (using discrete choice experiments)?
What aspects of quality of life are people with cancer willing to give up to increase their survival?
How long does it take people to return to work after a cancer diagnosis and treatment, and what makes it easier for them to do so?
When people stop working because of illness or injury, how can we measure the impact this has on the broader economy?
How do the costs of cancer treatment impact peoples emotional and physical well-being?
There are many opportunities for health economics to be used in occupational therapy, and I’ve included a list of examples at the end of this article. But three obvious areas would be: a) Economic evaluations, although a systematic review of economic evaluations in occupational therapy (Green & Lambert 2016) found only nine published economic evaluations (of varying quality), despite the increasing focus of health care systems on demonstrating cost effectiveness; b) Many occupational therapy interventions probably reduce future health resource use, so there are opportunities to use Medicare data (such as MBS and PBS payments) to examine the impact of occupational therapy (here is a good fact sheet on using Medicare data for research); and c) Discrete choice experiments (which quantitatively measure patient preferences) are an ideal method to examine people’s preferences for their health (e.g. which occupational domains they value most) and how they want their treatment delivered (e.g. what aspects of a rehab program make people most likely to adhere to a practice schedule).
Please feel free to get in touch if you have ideas or an interest in incorporating health economics into occupational therapy, of if there are other resources you’d like, or have found useful!
Examples of health economics in occupational therapy:
Hewitt et al (2018) An economic evaluation of the SUNBEAM programme: a falls-prevention randomized controlled trial in residential aged care [Link]
Kareem Brusco et al (2014) Are weekend inpatient rehabilitation services value for money? An economic evaluation alongside a randomized controlled trial with a 30 day follow up [Link]
Wales et al (2018). A trial based economic evaluation of occupational therapy discharge planning for older adults: the HOME randomized trial [Link]
Sampson et al (2014) An introduction to economic evaluation in occupational therapy: Cost-effectiveness of pre-discharge home visits after stroke [Link]
Laver et al (2012) Preferences for rehabilitation service delivery: A comparison of the views of patients, occupational therapists and other rehabilitation clinicians using a discrete choice experiment [Link]
Gallego et al (2018) Carers’ preferences for the delivery of therapy services for people with disability in rural Australia: evidence from a discrete choice experiment [Link]
I was thrilled to be awarded the Overall winner of the 2018 HSRAANZ Best Health Services and Policy Research Paper last night. These awards recognise the best scientific works in the field health services and policy research. The award was for my paper on cancer-related lost productivity in the developing countries Brazil, Russia, India, China and South Africa (see my blog post for more details).
The article impressed the judges in the scope of research undertaken and the value it will contribute to the research field, including its potential to guide local prevention and treatment strategies. (HSRAANZ)
For the paper I was responsible for leading a large, international team of researchers to conduct an analysis of productivity loss due to cancer in rapidly developing countries. I had a leading role in the conceptualisation of both the research question and the project methodology, and applied for and received funding through an EU CANWON fellowship to undertake the project. I gathered the necessary data with assistance from the international authors, and was solely responsible for the formal data analysis. As the lead author, I was also responsible for the project administration and preparation of the manuscript.
Following publication of the paper, I lead the promotion of the publication through various media channels, including The Conversation (~6,000 readers) and 44 radio, print and tv news articles (including The Guardian, Lancet Oncology News, UN News, 2SER ThinkHealth podcast, etc.) As a result, the article has gone on to be in the top 5% of all research outputs scored by Altmetrics, and the number 1 article of similar age published in Cancer Epidemiology. More importantly, I have worked with each of the international authors to ensure that the results have been disseminated to the appropriate policy and health service planning agencies and individuals in each of the BRICS countries. This has included developing country-specific specific results and graphs, assisting with presentation slides and encouraging broad dissemination lead by the other authors.
The above two paragraphs are a summary of the application I submitted to HSRAANZ for the award, and while it is true it skips the importance of this paper as part of my professional development. I was so lucky to be supported by Linda Sharp, Isabelle Soerjomataram and Paul Hanly to lead the research, and to apply for and take up funding to visit IARC and get the project started. The team we pulled together were really engaged with the project, and instrumental in pulling together and then interpreting the local and international data. I now count them as ongoing collaborators, and we already have a few papers and grant applications in the works.
But perhaps the most important lesson from this paper was resilience. I was so proud of this work once it was finished, but it took more than 12 months, an international relocation and 7 journal rejections before it was published. During that year I learnt perseverance and the value of a few days ‘cooling off’ before commencing the reformatting process, as well as how wonderful it is to have co-authors who will keep the faith in the manuscript alive when you (temporarily) run out! So thank you to everyone who helped out on the paper in whatever way – from digging out local data to offering supportive glasses of wine after another rejection! It was all worth it.
It is normal to experience distress after a cancer diagnosis, but for some people distress can become so severe it affects a person’s mental health. We found that people who have anxiety as well as cancer often cost the health system more, particularly when anxiety is undiagnosed and untreated.
Cancer patients with clinical levels of anxiety often cost the health care system more. This is because they often use more health resources, such as having more tests, or staying longer in hospital. While some of these extra resources might be to treat their anxiety, many are for physical complaints, and are incurred even when the anxiety has not been formally diagnosed.
For example, one study found that men with prostate cancer tended to opt for more intensive treatment if they had anxiety. Similarly, women with breast cancer were likely to stay in hospital longer, and have more complications, if they had a psychiatric disorder like anxiety. These extra days in hospital and treatment for complications meant their care cost the health care system an extra 13%. Similar results were seen for colon, cervical, head and neck cancers.
Given that more than 1 in 3 Australians will be diagnosed with cancer during their lifetime, finding ways to make cancer treatment more effective and more efficient is critical. Health services that improve the psychological support available to cancer patients could have long term cost savings, as well as providing improved patient care.
Despite how common clinical anxiety is, this review identified only five studies that looked at the costs of anxiety in people with cancer. Four were from Canada and the USA, and one was done in Germany.
Unsurprisingly, the studies that looked at treatments for anxiety found that health care use increased in the short term – often because patients accessed mental health support services. This meant that providing support for anxiety looked more expensive than standard care. However, no-one has looked at whether reducing anxiety among cancer survivors could reduce costs in the long term.
While most people diagnosed with cancer will experience distress, this is a normal reaction to a traumatic life event. However, at least 10% of people with cancer will have clinical levels of anxiety after their diagnosis. Young people, women and people with advanced cancer are particularly at risk. This anxiety can lead to feelings of fear, loss of control and avoidance, as well as physical symptoms such as poor sleep, headaches, and fatigue.
Even though there are effective treatments for anxiety, in the midst of cancer care, anxiety often goes undetected and untreated. One reason for this is that the physical symptoms of anxiety, such as, headache or stomach upsets are often attributed to non-mental health causes. Without appropriate treatment, anxiety can impair decision making and coping. It can also lead to poorer psychological and medical outcomes, including more side effects and poor treatment compliance.
The management of anxiety disorders in the cancer context is a clear example of where the evidence base for relatively low cost and effective methods for identification and treatment is available, yet not systematically implemented.
The full paper is available here: Joanne Shaw, Alison Pearce, Anna-Lena Lopez, Melanie Price. Clinical anxiety disorders in the context of cancer: A scoping review of impact on resource use and healthcare costs. European Journal of Cancer Care. https://onlinelibrary.wiley.com/doi/abs/10.1111/ecc.12893. Thanks to Jo Shaw for help writing this blog post.
Last week I attended the 2018 Women in Economics Retreat, organised by the Economics Society of Australia Women in Economics Network. It was 2 days in the Southern Highlands with a wonderful group of early and mid-career researchers, led by an amazing selection of mentors.
The attendees worked in a broad range of economics roles, including academia, government and consulting, and came from lots of different backgrounds (lots of closet architects among female economists apparently!) It was fascinating to hear how despite the varied ways we were all using economics, many of us faced the same issues.
I learnt a lot, met great people and came away inspired. Here are 5 great quotes I heard at the retreat, and why they resonated with me:
“Only 13% of economics professors are female … and … 9% of economists or analysts quoted in print media articles are female”. I come from a health background, and work in a centre led by fabulous female role models. These statistics highlight that my experience is not typical in economics, and something really needs to change. I’ll be taking small steps to try to increase the visibility of female economists in my circles.
“Everything is potentially really interesting”. We were talking about the value of having a growth mindset in the workplace, and I really liked the idea that there are opportunities all around us, if we can just adapt our mindset. Just because you don’t like a topic, doesn’t mean you can’t enjoy and learn from the methodology, or the team members, or something else about a project.
“In the spirit of Tony Jones, I’ll take that as a comment”. Day 2 saw us learning about Communicating with Influence. Rather than the standard media engagement strategies, this was practical advice given by the mentors. This quote was my favourite tip – about how to respond to that typical inappropriate / rambling / self-promoting interrupter in a seminar or conference presentation. I love that it (politely) puts the questioner in their place, while using the cultural reference to Q&A to keep it light and relax the audience. Hopefully I’ll never have to use it, but I feel more confident knowing I’ve got it up my sleeve!
“Done is the engine of more”. As someone who tends toward perfectionism, I’m a big fan of the mantra “Finished, not perfect” as a way to move myself on from tasks which don’t need to be perfect, but do need to be finished. I really like this alternative version because it highlights the benefits of finishing – not only do you get the task you’re working on done, but you can then accomplish more. I’ve printed this and put it on my office wall as a reminder!
“Distract daily, withdraw weekly, abandon annually”. The last session of the retreat was on work/life balance. This was fabulous, with practical and helpful ideas for everyone. Scheduling time to get away from work on a daily, weekly and annual basis makes so much sense, and it was fun and informative to hear how other people do this for themselves (and also really nice to know that I’m not alone in finding balance difficult to achieve!)
There was so much more that I learnt at the retreat, from stress coping styles to becoming good media talent, and from apps to encourage women to ask questions in conference sessions (Whova) to the importance of keeping a positive feedback log. One final thing I wanted to share was the various book recommendations that were suggested at different times over the weekend – I’ve listed them below.
I would highly recommend the retreat to anyone looking to develop a network of fantastic female economists, or who feels a bit stuck in their career and is wondering what their next move is. Congratulations to the Women in Economics Network for putting on such a great event.
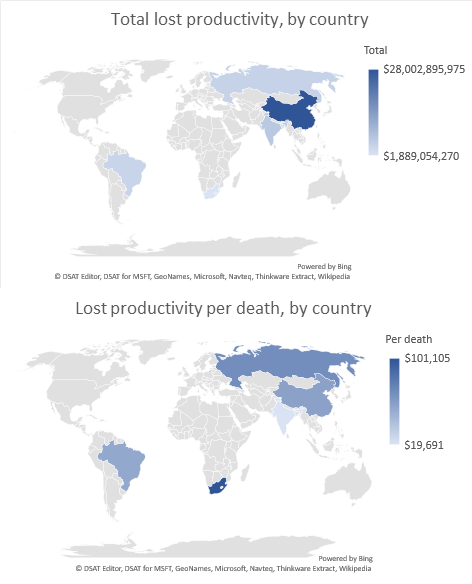
Premature – and potentially avoidable – death from cancer is costing tens of billions of dollars in lost productivity in a group of key developing economies that includes China, India and South Africa.
Over two-thirds of the world’s cancer deaths occur in economically developing countries, but the societal costs of cancer have rarely been assessed in these settings.
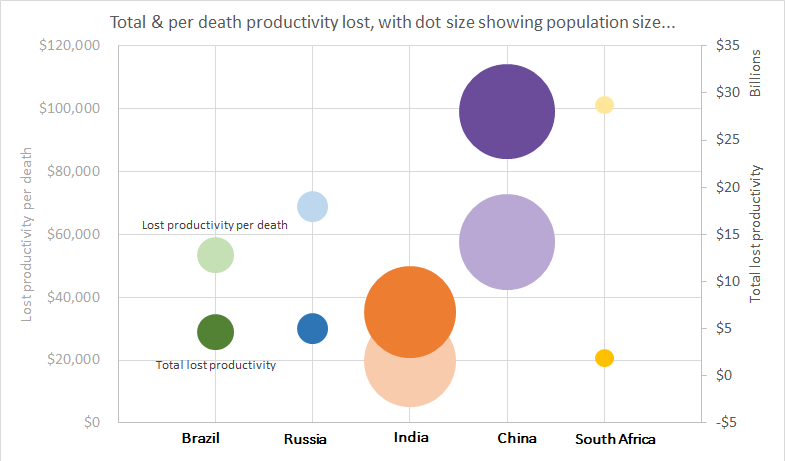
In a paper to be published in the journal Cancer Epidemiology we show that the total cost of lost productivity due to premature cancer mortality in Brazil, Russia, India, China and South Africa, collectively known as the BRICS countries, was $46.3 billion in 2012 (the most recent year for which cancer data was available for all these nations).
The largest loss was in China ($28 billion), while South Africa had the highest cost per cancer death ($101,000).
The BRICS countries are diverse but have been grouped by economists and others because of their particularly rapid demographic and economic growth. Currently the five countries combined comprise over 40% of the world’s population and 25% of global gross domestic product.
Liver and lung cancers had the largest impact on total lost productivity across the BRICS countries due to their high incidence, our research found.
But in South Africa, there are high productivity losses per death due to AIDS-related Kaposi sarcoma – an indication of the magnitude of the HIV/AIDS epidemic in Sub-Saharan Africa, and in India, lip and oral cancers dominated due to the prevalence of chewing tobacco there.
Many cancers which result in high lost productivity in the BRICS countries are amenable to prevention, early detection or treatment. Sadly, and in contrast to developed countries, most developing countries do not have such programs.
In particular, tobacco- and infection-related cancers (such as liver, cervical, stomach cancers and Kaposi sarcoma) were major contributors to productivity losses across BRICS countries.
Beyond the evident public health impact, cancer also imposes economic costs on individuals and society. These costs include lost productivity — where society loses the contribution of an individual to the market economy because they died prematurely from cancer.
Valuing this lost production gives policy- and decision-makers an additional perspective when identifying priorities for cancer prevention and control. This is particularly important in developing economies, where workforce and productivity are key resources in ensuring sustained economic growth.
Developing economies often have different demography, exposure to cancer risk factors, and economic environments than developed countries – all of which could modify the economic impact of cancer.
Locally tailored strategies are required to reduce the economic burden of cancer in developing economies. Focussing on tobacco control, vaccination programs and cancer screening, combined with access to adequate treatment, could yield significant gains for both public health and economic performance of the BRICS countries.
Country specific results
Brazil:
In Brazil, lung cancer resulted in the greatest productivity losses ($0.5 billion in 2012), with $402 million in lost productivity each year due to tobacco smoking, although Brazil has recently implemented successful tobacco use reduction policies.
Rapidly growing rates of obesity in Brazil result in up to $126 million in lost productivity due to cancer each year.
Russian Federation:
Total productivity lost due to cancer in the Russian Federation were $5 billion in 2012. They had the second highest cost per death of the BRICS countries.
Both liver and head and neck cancers contribute to the high number of excess alcohol-related deaths in the Russian Federation, with a likely considerably economic impact.
India:
Lip and oral cancers dominate lost productivity in India due to the relatively high prevalence of chewing tobacco. The use of smokeless tobacco, often combined with betel quid, may account for lost productivity of $486 million each year.
In India, the lost productivity costs per death of leukaemia are relatively high, perhaps because the advanced, multi-modality treatments required are not available, or are difficult to access
China:
Productivity lost due to cancer in China was $26 billion in 2012, more than all the other BRICS countries combined.
Two-thirds of total lost productivity costs in China were in urban areas (66%), considerably more than the proportion of people who reside in urban areas (52%).
In China, dietary aflatoxins in many staple foods is a major risk factor for liver cancer, and our results suggest this costs the economy $972 million annually.
South Africa:
In South Africa there are high productivity losses per death due to AIDS-related Kaposi sarcoma – an indication of the magnitude of the HIV/AIDS epidemic in Sub-Saharan Africa.
Cervical cancer represents a particularly large economic impact in South Africa. While there are new vaccinations available to prevent HPV, one of the precursors to cervical cancer, the effects of vaccination need a few decades to show impact. In the meantime, cervical cancer screening can offer an effective solution to reduce both the public health and economic burden of cervical cancer.
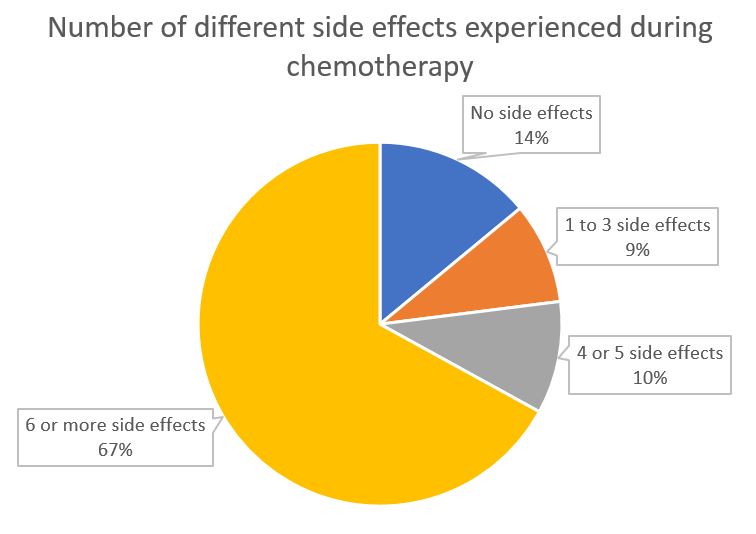
My latest publication shows that over three-quarters of people having chemotherapy in New South Wales experience multiple side effects during their treatment, and for over 60% of people this included a serious side effect. These results confirm previous research that suggests side effects might be more common, and more serious, in clinical practice (ie ‘real life’) than reported in clinical trials.
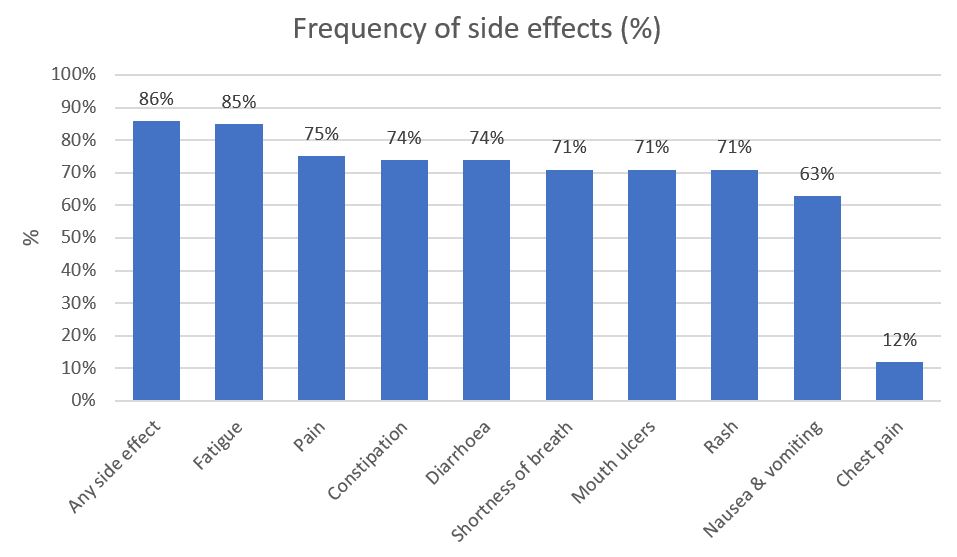
During their chemotherapy, 86% of our sample (who had lung, breast or colorectal cancer) reported at least one side effect, and 67% experienced six or more different side effects. Fatigue was the most common side effect (80%), followed by pain (75%), constipation (74%), and diarrhoea (74%). For nearly a quarter of participants (24%) the side effects were mild, but for many more (62%) the side effects were moderate or severe.
The number of different self-reported side effects experienced during chemotherapy by participants with lung, breast or colorectal cancer in the EOCC study
When we looked at the patterns of side effects over time, many people had mild side effects which stayed with them throughout their chemotherapy, especially constipation, diarrhoea, mucositis and nausea / vomiting. There was also a particularly large proportion of people reporting serious fatigue throughout their treatment.
The frequency of side effects self-reported side effects experienced during chemotherapy by participants with lung, breast or colorectal cancer in the EOCC study
The first study of this type in Australia, our Elements of Cancer Care study followed 441 people with breast, lung and colorectal cancer having chemotherapy in New South Wales. We interviewed them each month during their chemotherapy treatment to ask them about a wide range of topics, including what side effects they’d experienced and how serious they were. We also collected information from their medical records at the hospital and with Medicare.
Side effects in real life vs clinical trials
When new chemotherapy treatments are developed, the side effects they cause are tested in research studies called clinical trials. Doctors, patients and policy makers then base their decisions about chemotherapy on the data from these clinical trials.
But, what happens in clinical trials does not always reflect what happens in real life. Clinical trials usually have very strict criteria for who can participate. Clinical trial participants are usually younger and fitter than typical cancer patients, and so be more able to cope physically with chemotherapy and therefore less likely to have a side effect. In addition, clinical trials are usually conducted in large, high-quality, teaching hospitals with extra monitoring and treatment of side effects, which may reduce how often they occur, or how serious they become.
Asking patients about side effects
How patients are asked about side effects can also influence what they report. When doctors or nurses ask general questions like “how have you been feeling” or “have you had any side effects” patients might not remember or report all of their side effects, particularly if they are not still happening. We gave participants a checklist of side effects, which may have encouraged them to report a greater variety of side effects, and those side effects which were less severe. This is a technique which could be implemented by doctors and nurses in cancer care clinics.
What does this mean?
On top of dealing with a diagnosis of cancer and being treated with chemotherapy, having side effects can affect someone’s physical health, survival, quality of life and emotional state. Because our information comes from real life, rather than clinical trials, it allows doctors, nurses, policy makers and patients to think more realistically about the side effects of chemotherapy.
The Elements of Cancer Care study was funded by the National Health and Medical Research Council (Health Services Research Grant ID 455366). Alison was supported by a University of Technology Sydney Doctoral Scholarship, and a PhD top-up scholarship from NHMRC Health Services Research Grant (ID455366). Sallie is supported by a Cancer Institute NSW Career Development Fellowship (ID: 12/CDF/2-25). No funding organisation had any role in the study design, data collection and analysis, decision to publish or preparation of the manuscript.
Having just moved from Australia to Ireland to do a post-doc at the National Cancer Registry, I was interested in comparing the Australian and Irish cancer registration systems. Both countries have excellent cancer registries, with some similarities as well as differences between them. A table comparing the features of each system is below, but the primary differences are around the method of collecting data for the registry, and the amount of information captured.
In Ireland the Department of Health and Children has funded the National Cancer Registry Ireland since 1994. Cancer registration is not mandatory. However, data capture is close to complete through a system of active data collection through trained registry employees being stationed at hospitals around the country to collect cancer cases and data. Most new registrations are identified through the pathology report, however public hospitals also produce lists of cancer cases discharged each year, and death notices are checked as well. Six to twelve months after a new cancer notification, the tumour registration officer pulls the medical record for each notification, and completes the data entry. Information is collected on the individual, the cancer and their initial treatments, with the full data list provided in the registry manual (p9) here. Cancers are registered at the level of the individual, but are analysed at the tumour level.
In Australia, each state has an independent cancer registry, which reports a standardised minimum dataset to the National Cancer Statistics Clearinghouse at the Australian Institute for Health and Welfare (AIHW). The New South Wales (NSW) registry, managed by the Cancer Institute NSW, is described here as an example. Throughout Australia reporting of cancers (other than basal and squamous cell carcinomas of the skin) is mandatory, and whenever a hospital, pathology lab or radiotherapy centre deals with someone with cancer they are required by law to notify the cancer registry. Basic demographic, cancer and doctor information is obtained and supplemented with pathology reports and death certificates; however this is less extensive than in the Irish system. Cancers are registered at the tumour level.
Both registries produce very similar statistics such as incidence, prevalence and mortality rates, as well as specialised publications for topic areas of specific interest to the country. Data is made available by both registries to the government and other researchers, following appropriate ethical review and de-identification.
Table 1: Features of the Irish and Australian cancer registries compared
Feature
National Cancer Registry (NCR) Ireland
New South Wales (NSW) Central Cancer Registry
Australia Association of Cancer Registries (AACR)
Funding
Department of Health and Children
NSW Health through Cancer Institute NSW
Department of Health
Established
1994
1991. Dataset dates back to 1972
1982
Direction provided by
National Cancer Registry Board
Cancer Information and Registries Advisory Committee within Cancer Institute NSW
The AACR Executive Committee advises the AIHW on the direction of the National Cancer Statistics Clearinghouse (NCSCH) work program and the development of publication topics and strategies, and provides technical advice on the operation of the NCSCH.
Functions
to identify, collect, classify, record, store and analyse information relating to the incidence and prevalence of cancer and related tumours in Ireland
to collect, classify, record and store information in relation to each newly diagnosed individual cancer patient and in relation to each tumour which occurs
to promote and facilitate the use of the data thus collected in approved research and in the planning and management of services;
to publish an annual report based on the activities of the Registry;
to furnish advice, information and assistance in relation to any aspect of such service to the Minister.
act as a population based register of all cancers in NSW residents
monitor and undertake surveillance of new cases of cancer, survival and deaths in NSW
supply timely and accurate data based on a total record of all cases diagnosed in residents of NSW
analyse and report on the data in its national repository of cancer incidence and mortality statistics;
support research based on these data; and
develop and improve cancer statistics generally.
How are cancers registered
The reporting of cancer is not mandatory, however the NCR uses active ascertainment and follow up to ensure that there is accurate and complete recording of all cases diagnosed. Tumour Registration Officers employed by the registry are based at hospitals nationally. The main source of notification of new cases is a pathology report, however each public hospital provides a list of people discharge with cancer which is checked against the registry, as well as checking death notices and receiving notifications from registries in the UK.
All Australian states and territories have legislation that makes the reporting of all cancers (other than basal and squamous cell carcinomas of the skin) mandatory. State and territory population-based cancer registries receive information on cancer diagnoses from a variety of sources such as hospitals, pathology laboratories, radiotherapy centres and registries of births, deaths and marriages. When any of these institutions deal with someone with cancer, they are required by law to notify the cancer registries.
The cancer registry in each state or territory sends information to the National Cancer Statistics Clearing House at the AIHW to compile into a national database of cancer incidence, the Australian Cancer Database.Cancer data are also made available to the World Health Organization, state and local government authorities, health care institutions, health professionals and medical researchers.
What information is collected
The medical records are retrieved 6 – 12 months after notification to complete case information and capture relevant treatment information. Validation checks are performed at the point of entry and internal verifications are carried out monthly. See page 9 of the manual (www.ncri.ie/ncri/foifiles/Manual.doc) for details of data collected.
The CCR records new cancer cases and does not capture cancer recurrence.demographic information, brief medical details describing the cancer and a record of at least one episode of care. The data are supplemented by pathology reports and death certificates.
name and address
sex
date and country of birth
Aboriginal or Torres Strait Islander descent
clinical details about the cancer
the notifying institution and doctor
Definition of a cancer
Cancers are registered at the level of the individual, but are analysed at the level of the cancer. Metastasise are associated with the primary tumour and not considered separate cancers.
A case of cancer is the occurrence of a primary malignant neoplasm in one organ of a particular person. Therefore a case of malignant melanoma in an individual counts as one case. If the same person then develops leukemia, this counts as a second case.
This was a ‘cheat sheet’ I put together during the ACSPRI 2012 Winter Program course “Fundamentals of Multiple Regression” (Fun Reg). The cheat sheet simply summarises the concepts, formula’s and assumptions often used in regression analysis which were discussed in the course.
This was a fantastic course that I would highly recommend to anyone looking to use regression in their research. The course description is below for your information, and you can check out the full range of courses they run at http://www.acspri.org.au/courses
Fundamentals of multiple regression: This course provides an introduction to, and the fundamentals of multiple regression, covering enough of the statistical material for the intelligent use of the technique. The approach is informal and applied rather than emphasising proofs of relevant theorems. The course begins with a review of bivariate regression and extends the relevant principles to the case of multiple regression. Particular attention is given to the application of multiple regression to substantive problems in the social sciences. By the end of the course, the student will have a knowledge of the principles of multiple regression, and the ability to conduct regression analyses, interpret the results, and to inspect elementary regression diagnostics to test the underlying model assumptions. This course provides the foundations necessary for progression to ‘Applied Multiple Regression Analysis’, and to subsequent advanced-level courses in structural equation modelling and log-linear modelling.




 I was thrilled to be awarded the Overall winner of the 2018
I was thrilled to be awarded the Overall winner of the 2018 

{kind=link}
{kind=link}