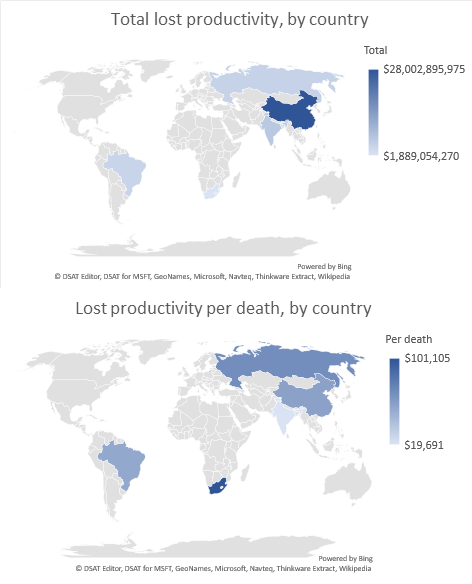
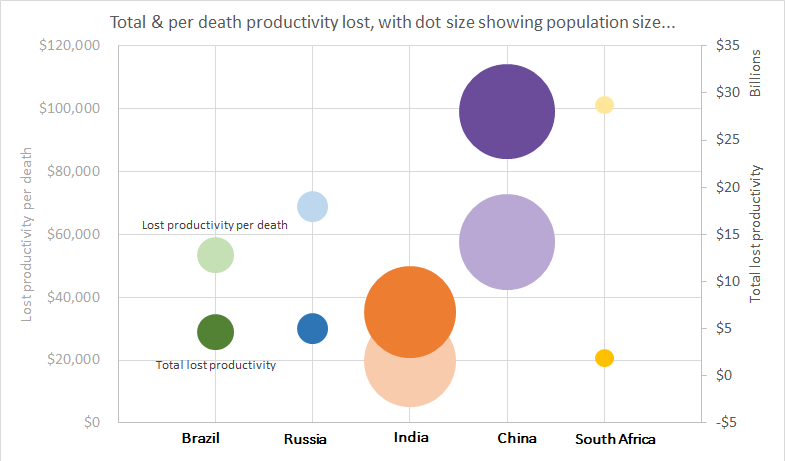
I was thrilled to be awarded the Overall winner of the 2018 HSRAANZ Best Health Services and Policy Research Paper last night. These awards recognise the best scientific works in the field health services and policy research. The award was for my paper on cancer-related lost productivity in the developing countries Brazil, Russia, India, China and South Africa (see my blog post for more details).
I was thrilled to be awarded the Overall winner of the 2018 HSRAANZ Best Health Services and Policy Research Paper last night. These awards recognise the best scientific works in the field health services and policy research. The award was for my paper on cancer-related lost productivity in the developing countries Brazil, Russia, India, China and South Africa (see my blog post for more details).
The article impressed the judges in the scope of research undertaken and the value it will contribute to the research field, including its potential to guide local prevention and treatment strategies. (HSRAANZ)
For the paper I was responsible for leading a large, international team of researchers to conduct an analysis of productivity loss due to cancer in rapidly developing countries. I had a leading role in the conceptualisation of both the research question and the project methodology, and applied for and received funding through an EU CANWON fellowship to undertake the project. I gathered the necessary data with assistance from the international authors, and was solely responsible for the formal data analysis. As the lead author, I was also responsible for the project administration and preparation of the manuscript.
Following publication of the paper, I lead the promotion of the publication through various media channels, including The Conversation (~6,000 readers) and 44 radio, print and tv news articles (including The Guardian, Lancet Oncology News, UN News, 2SER ThinkHealth podcast, etc.) As a result, the article has gone on to be in the top 5% of all research outputs scored by Altmetrics, and the number 1 article of similar age published in Cancer Epidemiology. More importantly, I have worked with each of the international authors to ensure that the results have been disseminated to the appropriate policy and health service planning agencies and individuals in each of the BRICS countries. This has included developing country-specific specific results and graphs, assisting with presentation slides and encouraging broad dissemination lead by the other authors.
The above two paragraphs are a summary of the application I submitted to HSRAANZ for the award, and while it is true it skips the importance of this paper as part of my professional development. I was so lucky to be supported by Linda Sharp, Isabelle Soerjomataram and Paul Hanly to lead the research, and to apply for and take up funding to visit IARC and get the project started. The team we pulled together were really engaged with the project, and instrumental in pulling together and then interpreting the local and international data. I now count them as ongoing collaborators, and we already have a few papers and grant applications in the works.
But perhaps the most important lesson from this paper was resilience. I was so proud of this work once it was finished, but it took more than 12 months, an international relocation and 7 journal rejections before it was published. During that year I learnt perseverance and the value of a few days ‘cooling off’ before commencing the reformatting process, as well as how wonderful it is to have co-authors who will keep the faith in the manuscript alive when you (temporarily) run out! So thank you to everyone who helped out on the paper in whatever way – from digging out local data to offering supportive glasses of wine after another rejection! It was all worth it.